Breathlessness is a very common distressing symptom in malignant and non-malignant disease. Up to 70% of patients with cancer experience breathlessness in the 6 weeks prior to death, and this may be greater in lung cancer patients because of co-existent COPD and right sided heart failure.
It is a frightening symptom for the patient and for those caring for them. There are specific resources for carers here.
Consider reversibility if appropriate
- Infection
- Lymphangitis - steroids may help
- SVC obstruction
- Heart Failure
- Pleural Effusion - consider drainage if well enough
Treatment options
Non–pharmacological interventions
- Keep room cool and open windows
- A hand-held fan blowing towards the face
- Pursed-lip breathing - inhale through nose with mouth closed, then exhale slowly through pursed lips for 4 to 6 seconds.
- Sitting upright and lean forward with arms bracing a chair or knees
- Visualisation and complementary therapy
- Nutritional advice e.g. small frequent meals, easily chewed
- Anxiety management
- Social interaction eg Breatheasy groups
Opioids
- Relieve the sensation of breathlessness - there is much evidence of efficacy and safety in doses of less than 20mg per day
- Start low and go slow e.g. immediate release oral Morphine (e.g. Oramorph®) 2.5mg–5mg P.R.N., then regularly 4-6 hourly if beneficial
- Even lower doses may help if elderly or frail e.g. 1mg to 2mg oral Morphine
- Long-acting opioids can be very effective and are safe e.g. Morphine Modified Release Tablets 5mg bd
Benzodiazepines
- Useful for those patients with anxiety/panic associated with episodes of breathlessness
- Less evidence for efficacy than opioids in relieving breathlessness
- e.g. Lorazepam (1mg blue tablet – Genus or Teva brand) 0.5mg sublingual 4–6 hourly P.R.N.
For patients already on opioids
Lower opioid dose needed than breakthrough analgesic dose is often sufficient for breathlessness, e.g. 25-50% of the current PRN analgesic dose.
Oxygen
Limited value if oxygen saturation is already >92%. However some patients find the work of breathing is eased by Oxygen even if if oxygen saturation is good.
Breathlessness in the last days
- Continue non-pharmacological treatments
- Morphine 2.5 mg to 5 mg and Midazolam 2.5 mg -5mg subcut P.R.N. for repiratory distress (a syringe pump may help if several injections are needed)
- Morphine 10 mg over 24 hours via a syringe pump, increasing stepwise to Morphine 30 mg over 24 hours as needed (start with 5mg if very frail)
- Midazolam 10 mg over 24 hours via the syringe driver, increasing stepwise to Midazolam 30 mg over 24 hours as required (start with 5mg if very frail)
- Consider 20-40mg furosemide subcut or an infusion as pulmonary oedema may be contributing
- Consider treating retained secretions (death rattle)
Key Points
- Do contact the local specialist palliative care team for more specific advice
- Lower starting doses in frail elderly and those with renal failure
- Non-drug methods to relieve breathlessness are crucial
- Identify and treat reversible causes of breathlessness
- Consider an opioid and benzodiazepine combination for patients at the end of life
- Sedation and opioid use should not be withheld because of a fear of causing respiratory depression. The intention is to relieve respiratory distress, not to hasten death
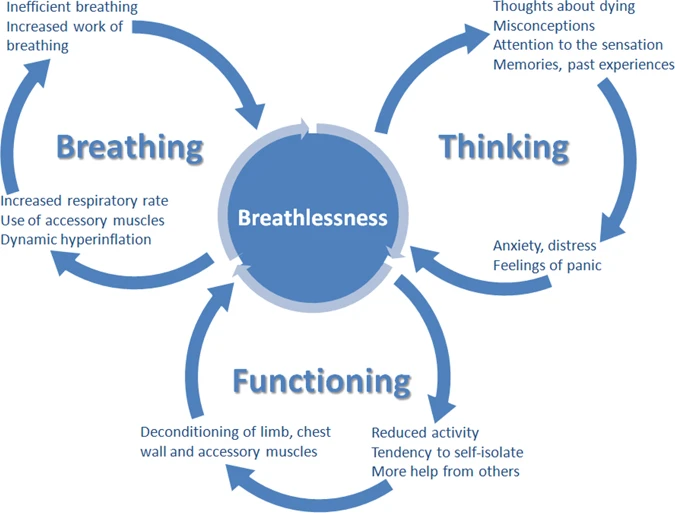
Chronic breathlessness syndrome is breathlessness that persists despite optimal treatment and can be managed with the Breathing, Thinking, Functioning holistic approach: